Strategic Trends in Manufacturing and Distribution
Off The [Cold] Chain: New Ideas For Managing Ultra-Cold COVID Vaccines
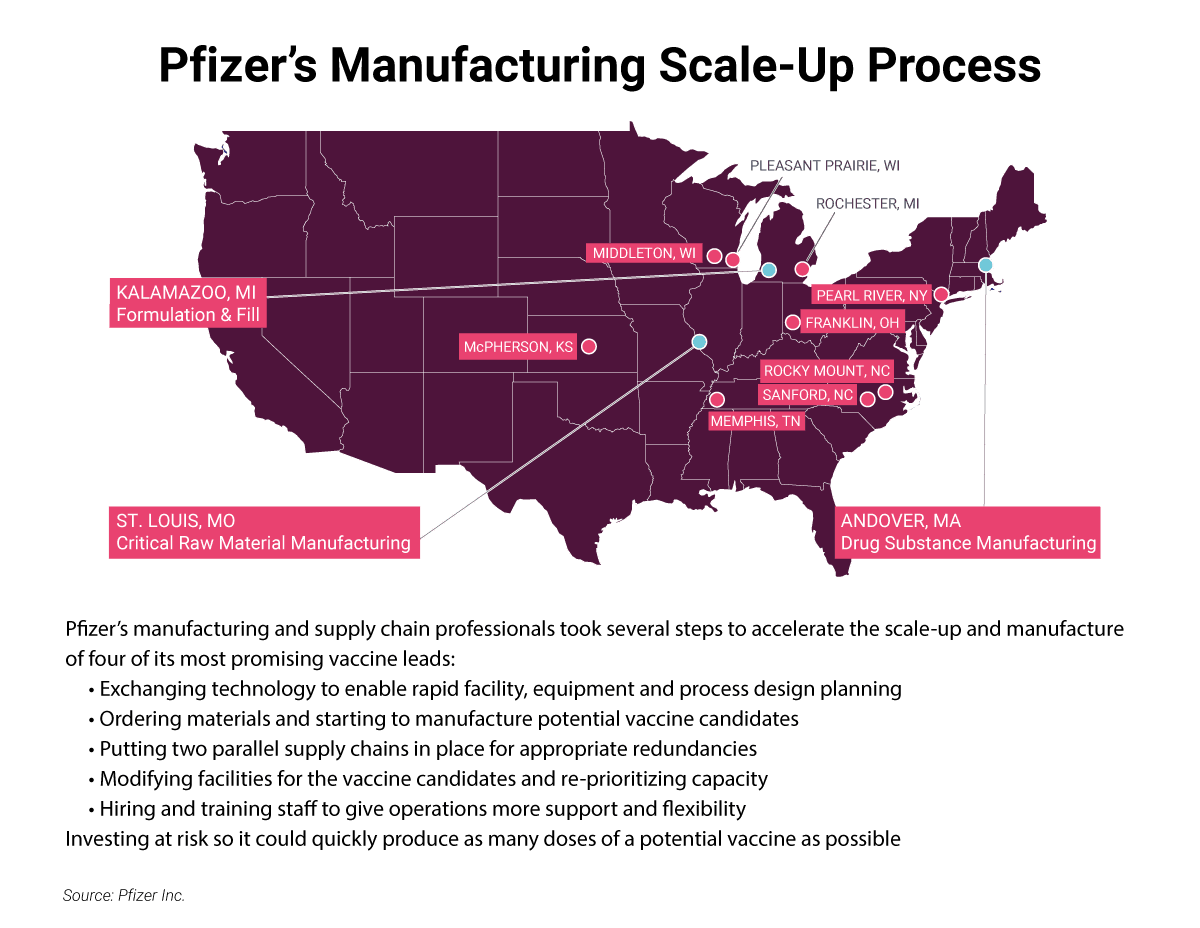
At War With A Pandemic: Manufacturing For Our Lives
Could Automation Rescue CAR-T Manufacturing?
Solutions Exist To Regenerative Medicine's Most Pressing Manufacturing Challenges
Merck & Co, Indian Firms On Tackling Supply Chain Risks And A Hijack
A Biopharma A-List Lineup Aims To Tackle Complex Manufacturing At Resilience
Off the grid ultra-cold storage “Vaccine Pods” and mRNA vaccines reformulated to be stable at room temperature are two innovative ways to address the problem of getting the whole world vaccinated against COVID-19.
When Larry Davis recorded “Texas Flood” in 1958 – “Well it’s floodin’ down in Texas/all the telephone lines are down” – he probably never imagined that a blizzard would knock them out in 2021. And not just the telephone lines. During the historic snowstorm in February, the Texas Department of State Health Services announced that thousands of COVID-19 vaccines would not arrive as planned, due in part to concern about power outages and the potential for vaccine spoilage. Even if the vaccines did arrive on time, people might not be able to travel to vaccination sites.
It does not take a blizzard to interrupt the cold chain infrastructure needed to keep vaccines at the correct temperature, from manufacturing site to injection. And it is not clear how many COVID-19 vaccines have been wasted so far. In the US, the CDC requires vaccination sites to report the number of wasted doses, but some state governments are not complying, according to reporting from ProPublica. Many states, however, have reported thousands of wasted doses, due to problems maintaining ultra-cold refrigeration, broken vials or other shipping issues.
Globally, the World Health Organization estimated that 50% of vaccines are wasted each year, due to inadequate temperature control and shipping problems. In the world’s poorest countries, only 10% of health care facilities have a reliable electricity supply, according to GAVI, the Vaccine Alliance. GAVI’s Cold Chain Equipment Optimisation Platform, established in 2016, is working to upgrade cold chain infrastructure in the 57 countries eligible for vaccine support, but many challenges remain.
Edward Collins, a retired firefighter and battalion chief, a former CEO of a national retail mattress chain, a real estate agent and a bar owner based in Kansas City, Missouri, wanted to help when COVID-19 struck. In an interview with In Vivo, Collins said he had lost three friends in the fire department to COVID-19, and the virus was a contributing factor in his wife’s death last year. “At the beginning they said we’d need ventilators. I went to Home Depot [a home improvement retailer] and Micro Center [a computer and electronics retailer] and made a homemade ventilator for $88,” said Collins. “I published those plans for free on a website for COVID-related products … but then there wasn’t the rush on ventilators like everyone thought, but I just wanted to help.”
Edward Collins, Founder and CEO, Vaccine Pods
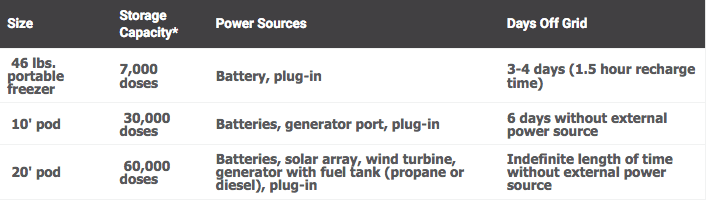
Next, Collins started looking at the supply chain for products requiring ultra-cold storage. “If you look from the manufacturer to the end user, it’s fraught with all kinds of problems,” said Collins. “We’re talking about saving billions of lives, and we’re entrusting that to cardboard boxes with dry ice … you can recognize the breaks almost immediately.” He considered producing dry ice, or opening up freezer farms in existing facilities to assist the supply chain, but ultimately decided to launch a new company from stealth – Vaccine Pods – on 27 January, 2021. Through a partnership with HCI Energy LLC, a power solutions company, and Stirling UltraCold, an ultra-low temperature freezer company, Vaccine Pods are shipping containers capable of storing vaccines safely with or without an external power supply (see Exhibit 1).
Exhibit 1. Vaccine Pod Options And Specifications
Source: Vaccine Pods
*Vaccine dose capacity numbers vary slightly according to product type
The partnership with HCI Energy, also based in the Kansas City area, came about serendipitously: Collin’s patent attorney also had HCI Energy as a client, and connected Collins with HCI Energy CEO Ray Ansari. “It made sense to bring in [HCI Energy] as a strategic partner with us to provide their technology base, and pair it out to Sterling UltraCold’s freezers, and have the whole package put together in the Vaccine Pods,” said Collins. During the discovery phase of putting the
company together, Collins realized that Stirling UltraCold “was the only commercial grade lab freezer in the world capable of reaching the temperatures we needed, but also adjustable to a broad range of temperatures to accommodate every vaccine coming out.” Stirling UltraCold sold Collins a demo unit from one of its showrooms, and he brought it to Kansas City. There, Collins combined the technology from HCI Energy and Stirling UltraCold together, inside the pod.
The Vaccine Pods are available in 10-foot and 20-foot models, with an additional “rapid intervention freezer,” a Stirling UltraCold portable freezer ULT-25 model. All three models are equipped with telemetry systems for monitoring freezer health, temperature, ambient temperature inside the 10’ and 20’ pods, solar wattage produced, power levels inside the pod, and fuel levels inside of the back-up generator, said Collins. “We have 24-hour real-time monitoring for all of this, which allows us to dispatch fuel trucks against a client’s fuel count if needed, to maintain power at all times.”
Vaccine Pods can be transported on “planes, trains and automobiles,” said Collins, including roll-off tow trucks, gooseneck trailers and flatbeds, and they are also rated for cargo ships and can be stacked, “even with the solar array tucked away on the inside.” The pods are capable of withstanding 145 mile-an-hour winds, and are locked down on site, once in place. The 20’ pods having air conditioning and heating systems and can turn a parking lot into a vaccine administration site. “People can drive up to them, come in, we can install a table inside [the pod] and give vaccinations right there,” said Collins. Security keys and codes are used for access, which can also be granted remotely. Vaccine Pod security is “not quite to the level of a Brink’s Truck, but it’s pretty close.”
Collins believes his initial customers will be government agencies and NGOs. “We’ve had great conversations in Washington DC, with congressmen and congresswomen, and they hand-walked our units over to multiple agencies focused on vaccine deployment and vaccination plans,” said Collins. “We’ve had incredible outreach from local governments, health departments, bureaus of federal prisons,” as well as NGOs such as USAID, UNICEF and the Gates Foundation. “Hopefully, as we get through communication and discussions with people in DC, we can lump everybody under the Defense Production Act to assure that we have the supply chain we need to fill everybody’s order.”
Pricing for the Vaccine Pods ranges from $38,000 to $40,000 for the portable rapid intervention freezer, which holds 7,000 doses and can go off-grid for three to four days before recharging. The 20’ pod, which can hold two 30,000 vaccine capacity Stirling freezers, for a total of 60,000 vaccines, with “all the bells and whistles, including redundant power supply, and depending on how many batteries you include, comes in at about $189,000,” said Collins, estimating that 30,000 doses might be worth around $6m, making extra power redundancies a sound insurance policy.
After COVID, Collins hopes to expand into different areas. With the launch of mRNA vaccines, “we are going to have ultra-low temperature vaccines for a long time, and they will expand into different areas,” said Collins. “But we’re also looking at any [drug] that requires any type of refrigeration or freezing. Whether it’s an mRNA vaccine or more traditional vaccines, we’ll be able to go forward and help with other inoculations like rheumatic fever and polio in remote areas of the world.”
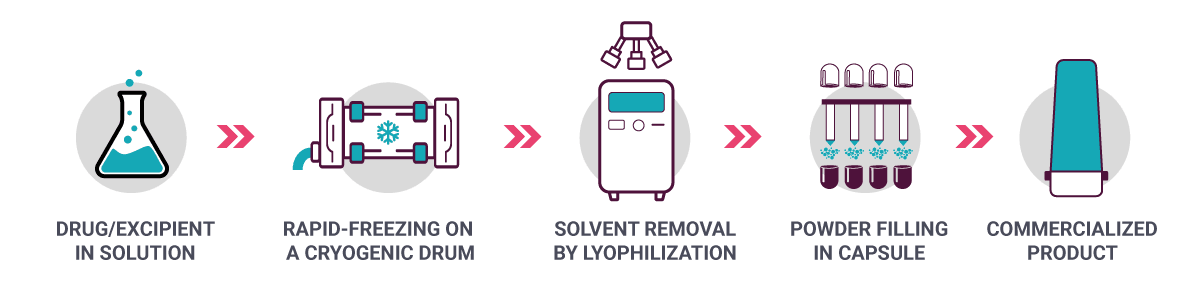
What if vaccines – and monoclonal antibodies, for that matter – no longer needed to be refrigerated, and remained stable at room temperature? Robert O. Williams III, inventor of thin film freezing technology (TFF) and scientific consultant to TFF Pharmaceuticals, is hoping to accomplish just that. In an interview with In Vivo, Williams, who is also head of the College of Pharmacy’s Molecular Pharmaceutics and Drug Delivery Division at the University of Texas at Austin, said TFF technology began as a research collaboration 20 years ago with the Dow Chemical Company. “We were interested in an alternative delivery route for drugs, including biologics, so that we could get them to the lungs,” said Williams. TFF technology is created through a process involving rapid freezing in a cryogenic drum and lyophilization (see Exhibit 2).
Exhibit 2. Thin Film Freezing: From Liquid To Inhaled Powder
Source: TFF Pharmaceuticals
Today, TFF Pharmaceuticals, based in Austin, TX, is carrying that project forward. “We started working on technology about five years ago specifically for biologics like the mRNA-based vaccines,” said Williams. “It’s fortunate that we did, because now we’ve built up a significant amount of know-how and intellectual property and publications on applying thin film freezing as an alternative for stability storage, which doesn’t require cold chain.” Even before the advent of mRNA vaccines, refrigeration has always limited biologic distribution, particularly in countries without advanced cold chain storage capabilities,” said Williams. “COVID-19 vaccines have brought the seriousness of this issue front and center.”
While TFF Pharmaceuticals has not tested its technology on the Pfizer/BioNTech and Moderna mRNA vaccines specifically, the company has tested it on “several different mRNA [products] contained in lipid nanoparticles … We are working with those now and have had successful results with applying thin film freezing to stabilize mRNA lipid nanoparticle-based therapeutics,” said Williams. “They’re similar to the [BioNTech and Moderna] vaccines, and directly applicable.” TFF Pharmaceuticals has not disclosed which mRNA products it is testing with TFF technology but has described its partners as “the top pharma companies in the world,” said Williams.
TFF Pharmaceuticals has also developed an inhaled formulation of Veklury (remdesivir), Gilead’s antiviral therapy, which received FDA approval on 22 October, 2020 for patients with COVID-19 requiring hospitalization. The approval followed an Emergency Use Authorization last May. Williams developed the inhaled remdesivir formulation in his lab, sponsored by TFF Pharmaceuticals, and said it “works really well … we just completed a study in hamsters, the preferred COVID infection animal model, and have recently published a paper [on those results].”
Williams believes that an inhaled formulation of remdesivir offers “a lot of benefits over the intravenous form currently approved, and what we believe is a nebulized form of remdesivir that Gilead has stated publicly that they are developing and testing.” The question now for TFF Pharmaceuticals is whether and how to move the program forward, given that Gilead has a patent on the raw material. “We’d like to partner with them, so that’s where it stands,” said Williams. TFF Pharmaceuticals also announced a joint development and collaboration agreement with Augmenta Bioworks on 2 November, 2020, to reformulate select Augmenta monoclonal antibodies into inhaled treatments for COVID-19.
Robert O. Williams, inventor of thin film freezing
In press materials, TFF Pharmaceuticals announced that it has identified 18 potential drug candidates that could be transferred to inhaled or oral formulations. The company has a partnership with Denmark-based UNION Therapeutics to develop an inhaled formulation, and an “improved” oral formulation of niclosamide, an antihelminthic drug used to treat parasitic infections, and with potential applications in a range of other diseases. Last October, the company announced “positive preclinical immunogenicity and efficacy data” from TFF formulated “universal influenza hemagglutinin recombinant vaccines,” through a partnership with the University of Georgia’s Center for Vaccines and Immunology.
Williams said TFF Pharmaceuticals aims for “room temperature storage for two to three years for a typical kind of pharma product.” With biologics, “when you have a dry powder that has the properties of our TFF process powder, we have examples of vaccines and examples of different proteins where we are able to go out for about a year and half or two years now, with stability that we’re following. Every molecule is unique, but that’s our goal, and we think it’s achievable.”
The benefits of TFF formulation could go beyond room temperature storage, explained Williams. “For each type of active material, whether it’s niclosamide, or a monoclonal antibody, or the influenza vaccine, they are nuanced amongst themselves.” But the key benefits may come in the form of lower dosages, and a reduction in off-target side effects. That had been demonstrated in hamster models with respect to TFF formulated niclosamide, said Williams.
For many in the biopharmaceutical industry, inhaled biologics will immediately call to mind the twin failures of Pfizer and Mannkind’s inhaled insulin products, which ultimately spooked physicians and patients over pulmonary risks. Williams acknowledged that risks have to be determined case by case during the clinical process, but said “a lot has been learned about applying the different larger molecules like proteins and peptides into the lungs” since the excitement around inhaled insulin. “With TFF Pharma, we’ve talked to 30 or 40 companies now, and the scientists – I’m generalizing – but the scientists that I talked to are not concerned about [pulmonary risks] now. They think there's always a risk, but it's one worth taking to apply these biologics into the lung. Their limiting factor has been that they didn't have a way to do it, because there was no way to form an inhalable powder with a biologic that preserves the biologic's chemical integrity, its activity. But we can do it with thin film freezing technology.”
The rapid development of a vaccine to fight COVID-19 is an effort that will be discussed and admired for centuries to come. The effort to make and deliver the vaccines to those who are most at risk is a battle all of its own. Two manufacturers talk to In Vivo about managing roll out strategies when the whole world is watching.
“Never was so much owed by so many to so few,” the infamous quote attributed to wartime leader Winston Churchill, referring to the pilots that engaged in the Battle of Britain, has never been more applicable to a modern situation than the one we are facing globally today. Indeed, the world is at war again. This time, the enemy is a mutating virus that has brought industry and education to a standstill. This time, “the few” we must thank for standing up to the enemy, and giving the world back its normalcy, are the chemists, scientists and manufacturers behind the COVID-19 vaccines that have been approved and are still in development.
Never has the biopharmaceutical industry been asked to move so fast to counter a global health crisis. According to Bloomberg data at the end of February 2021, more than 231 million vaccine doses had been administered across 88 countries. The latest rate was roughly 6.35 million doses a day. As of the end of February, the UK had vaccinated 25% of its population, with a target to offer a vaccine to all UK adults by 31 July, 2021 . In the US, for the last week of February, an average of 1.45 million doses per day were administered.
Behind these remarkable figures is a tireless manufacturing wheel that keeps on turning. While the pharmaceutical industry remains entrenched in the quagmire of the pandemic, it may be too early to take stock of the lessons learnt. However, there are ways in which manufacturers of the vaccines have operated that deserve to be applauded.
Clive Glover, director of strategy at Pall Corporation and the lead on manufacturing strategy for Oxford University and AstraZeneca PLC’s AZD-1222 vaccine project, told In Vivo that while the speed of the manufacturing process has been remarkable, it has “not been easy.”
The COVID-19 vaccine was co-invented by the University of Oxford and its spin-out company, Vaccitech. It uses a replication-deficient chimpanzee viral vector based on a weakened version of a common cold virus (adenovirus) that causes infections in chimpanzees and contains the genetic material of the SARS-CoV-2 virus spike protein. After vaccination, the surface spike protein is produced, priming the immune system to attack the SARS-CoV-2 virus if it later infects the body.
The speed at which the AZD-1222 vaccine has been manufactured is significant. Within eight weeks, Pall Biotech designed the manufacturing process to deliver millions of doses per batch, then delivered and installed the equipment the contract manufacturing partner would need to make the vaccine.
The first manufacturing run began less than two months after Pall received the starting material from Oxford University. To put this into context, Pall’s previous record for this process was nine months. Glover said this action required a combination of ground-breaking innovation, huge amounts of funding, relentless effort from some of the greatest scientific minds on the planet and, crucially, a consortium-wide commitment to the principles of lean process development and production.
As the scale of pandemic became apparent, Oxford University put out an open call for process development capabilities to scale up the manufacturing process to make millions of doses. “Pall responded to this call as we have our Integrated Solutions team located in Portsmouth, UK,” explained Glover. The Integrated Solutions team routinely develops these kinds of processes for clients. In the last three years, Pall Biotech has developed more than 30 processes for clients and most of its expertise is around developing large scale viral vector manufacturing capabilities. This fit very well with Oxford University, as its vaccine is based on an adenovirus.
Oxford University only had a small-scale manufacturing process worked out. It provided the initial starting materials and guidance to the Pall team who then took this and developed the large-scale manufacturing process. At the same time, Pall was in constant contact with the contract manufacturing organizations to ensure that the process Pall had developed would fit into their facilities, and to coordinate Pall’s supply chain with their availability. Pall tech-transferred the process to three CMOs; UK companies Cobra Biologics and Oxford Biomedica, and Halix based in the Netherlands. The Vaccine Manufacturing and Innovation Centre also provided invaluable logistical coordination and advice to the whole team, added Glover.
In total, at Pall there were about 20 people that worked on the project full time for eight weeks, but they were supported by many others, and several of them continue to support the manufacturing process today. The Integrated Solutions team consists of the Process Development Services lab and the Engineering team. These two teams work together very closely. Together they suggested technologies that could be used to manufacture the vaccine at scale. The Process Development Services team then tests these technologies on a small scale initially and then at full manufacturing scale to ensure that the process works as planned.
Crucial process data is also captured at the time to help with future regulatory filings. Once the Process Development Services team have demonstrated that the proposed technologies work at scale, the Engineering team takes the process, puts together a full equipment list and designs all the required single-use manifolds that are essential to tie the process together. It also ensures that the equipment will fit in the clients’ facility. Once the process has been tested and the facility designed, the client gets final approval. In parallel to this, Pall’s supply chain team becomes involved to ensure that it can deliver both the equipment and the single-use components on time.
“The key to the rapid development of this process is that we did not design it from scratch,” said Glover. While every product has its own unique requirements, the backbone of the process remains consistent for each viral vector. “We use the 80/20 rule here: 80% of the process is common but it does require the final 20% customization both because of the individual product and also because of the specific facility that the process needs to be fitted into,” he explained. Two years previously, Pall had developed a standardized viral vector manufacturing process. “We had already worked out this process in a high degree of detail and it was to this was that we turned when required to develop this process,” he recalled.
This was a complicated project with many different stakeholders including Oxford University, the three CMOs as well as the UK government. AstraZeneca became involved in the process in early May 2020 to take the vaccine global. “This was all taking place just as we were all getting used to working from home so that really complicated matters. Adding to that, social distancing in a process development lab can be difficult particularly when two people may be required in some parts of the process,” recalled Glover. “Furthermore, our supply chain had to be operating at full capacity in order to get equipment and consumables together in a timely manner. However, there was a very singular and urgent focus to the team, and through taking the correct safety precautions, the team in the lab were able to collaborate which enabled us to work through issues that arose quickly and efficiently.”
Glover describes the supply chain efficiency offered by Pall Biotech as a “normally well-oiled machine.” However, the Oxford-AstraZeneca vaccine was of course not the only vaccine in development. In fact, at that time there were more than 200 different vaccines and therapeutics in development and many of them were also requesting urgent supplies from Pall Biotech to support those efforts.
One of the crucial things Pall did was to rely on the standardized viral vector manufacturing process. “The standardized process allowed us to harmonize single-use consumables across multiple manufacturing sites. This, in turn, gave our supply chain fewer part numbers and designs to have to work on and increased the volume on particular designs allowing us to manufacture these in bulk,” he explained. “This has the advantage that it considerably reduces the supply chain risk with any single part, which is very important.”
This became even more critical for the project as the vaccine went global. AstraZeneca is now working with more than 20 different manufacturing partners globally and needs to be able to produce more than three billion doses. “Minimizing risk in the supply chain at this scale is essential,” affirmed Glover.
“The challenges we have faced setting up production lines are mainly linked to the extremely compressed timelines,” explained André Goerke, business unit head, mRNA, at Lonza, a service provider manufacturing active pharmaceutical ingredients and innovative dosage forms for the global industry.
The timeframe meant sourcing equipment and raw materials as well as hiring and training new staff in record time, Goerke told In Vivo. “There are more than 400 raw materials that we need to bring together and we are working closely with Moderna, Inc. and suppliers. A very frequent governance with all suppliers has been key. We are monitoring certain key compounds, their availability and projections on a daily level. All of our suppliers are aware of the importance of our needs and we try to jointly anticipate potential bottlenecks, to enable timely ramp up of production.”
In May 2020, one of the vaccine front runners, Moderna, announced a 10-year strategic collaboration with Lonza as its drug substance manufacturing partner for Moderna’s vaccine messenger RNA (mRNA-1273) vaccine. This was the first collaboration of its kind between Moderna and Lonza and allowed Moderna to accelerate its manufacturing capacity 10-fold.
The goal of the collaboration is to enable the manufacturing of up to one billion doses per year. The manufacturing process was developed by Moderna and the tech transfer began a month later, in June 2020, with the first batches of mRNA-1273 manufactured at Lonza’s Portsmouth, New Hampshire, plant in July 2020.
“The manufacturing of Moderna’s COVID-19 vaccine in Visp, Switzerland, takes advantage of the Lonza Ibex Solutions facilities,” explained Goerke. “Two years ago, Lonza made a considerable investment into flexible and technology agnostic manufacturing shells,” he said. These pre-built shells are already linked up to central infrastructure and services (including analytics and quality control labs) and allows Lonza to drop in the manufacturing technology that is needed for a particular drug or vaccine. “This is important,” he said “given that vaccines and drugs are becoming more diverse and a facility for one drug or vaccine cannot be easily used for another type of molecule. By using prebuilt shells, we have been able to set up dedicated facilities for mRNA production in less than eight months, compared to the two or more years it would take to set up a new facility from scratch.”
Today, the vaccine is made from one manufacturing line in Portsmouth and three lines in Visp. Globally, several hundred people work on the manufacture of the vaccine. “Compared to traditional biotech, this manufacturing platform is extremely efficient; many doses can be produced with a relatively small manufacturing footprint and number of staff,” said Goerke.
Approximately 60 million doses globally, including approximately 55 million doses to the US government, have been shipped to date and the first four million doses shipped from Modern’s ex-US supply chain.
An additional 33 million doses have been produced in the US, have been filled in vials and are in the final stages of production and testing before release. Moderna expects to complete delivery of the first 100 million doses to the US Government by the end of the first quarter 2021, the second 100 million doses by the end of May 2021 and the third 100 million doses by the end of July 2021.
Production planning during a pandemic is uncharted waters. New variants of coronavirus mean that a one-size-fits-all approach is not the end of the story. At the end of February, Moderna announced new capital investments to increase capacity at its owned and partnered manufacturing facilities, which it expects will
increase global 2022 capacity to approximately 1.4 billion doses of its COVID-19 vaccine, assuming a 100 μg dose. The investments will enable additional production of the current vaccine and provide flexibility in addressing production of potential vaccine boosters that may be needed to address emerging variants of SARS-CoV-2.
While the 2022 capacity of up to 1.4 billion doses reflects an assumption of a 100 μg dose, the 2022 output will depend on the dose of the booster. Moderna plans to study a dose range of 50 μg and lower for variant-based boosters and an additional booster of mRNA-1273. If the effective dose for a booster is 50 μg, then the 2022 supply could be significantly higher than 1.4 billion doses.
The company said it is “continually learning and working closely with its partners and the federal government to identify ways to address bottlenecks and accelerate production.” For example, one of the recently identified constraints on production has been the capacity of the fill-and-finish process. Moderna has now studied the possibility of adding more doses to each vial of vaccine to allow complete manufacturing to run more quickly and reduce the need for consumable materials that are in high demand. The FDA has provided positive feedback on this proposal, and Moderna said it is pursuing a plan that may allow up to 15 doses to be drawn from each vial. This will allow the production and delivery of additional doses more quickly.
Increasing production is also on the mind of other vaccine producers. AstraZeneca and the German contract development and manufacturing organization (CDMO) IDT Biologika have announced they intend to “explore options” to accelerate output of finished vaccines in the second quarter of 2021. The companies are making an undisclosed joint investment to build large additional drug substance capacity at IDT Biologika’s production site in Dessau, Germany. They will build up to five 2,000-litre bioreactors capable of
making tens of millions of doses per month of AstraZeneca/Oxford’s COVID-19 vaccine, estimated to be operational by the end of 2022.
The investment could also allow for the manufacture of other vaccines sharing a similar manufacturing process, greatly expanding Europe’s domestic vaccine production capability, said the companies in a joint statement. “IDT Biologika will have among the largest vaccine manufacturing capacities of its kind in Europe and play an important part in ensuring Europe’s future vaccine supply independence.”
Of course, not all vaccine manufacturing and delivery has gone smoothly. At the end of January, a diplomatic tussle broke out in Europe over a shortfall in projected vaccine doses from AstraZeneca’s Belgian plant. Local health authorities inspecting the factory in Senneffe after a “glitch” with the manufacturing process brought the promised 80 million doses down to 31 million. AstraZeneca CEO Pascal Soriot said that the Novasep plant had experienced low yields, which was to be expected as worldwide production was scaled up so rapidly in such a short space of time.
Commenting at the time, Novasep said that manufacturing the COVID-19 vaccine is a “pioneering process in terms of scale, complexity and quantity.”
Because the UK’s supply of the vaccine was undisturbed the European Commission demanded doses of the vaccine be sent from British manufacturing plants to make up for the shortfall. The UK government resisted the pressure and insisted that its orders must remain in Britain.
However hard manufacturing during a crisis is, planning during one is equally difficult.
Manufacturing constraints have prevented even the most pioneering cell therapy companies from meeting patient demand for their life-saving treatments. They are still in the works, but could fully automated, closed manufacturing platforms be potential game changers?
The advent of cell therapies holds the promise of new cures and treatments, but the roll out of these high-
cost medicines to eligible patients has been underwhelming to date.
This is largely due to manufacturing constraints that are peculiar to this sector. Cell therapies cannot benefit from the economies of scale because they are personalized, and their production process starts and stops with every individual patient.
To say that the manufacturing of cell therapies is complex and costly is an understatement – it takes highly-specialized staff around two weeks to produce one drug for one patient and the manual effort involved in the process is staggering.
Recent manufacturing innovations have resulted in some of the manual sub-steps being replaced with automated solutions, but there is still a tremendous amount of human labor involved overall. As a result, the industry is struggling to keep up with supplies and the cell therapies remain costly.
Even the very best and most pioneering companies in this field are not meeting patient demand for their revolutionary treatments. “They are not even close. They're [meeting] maybe 10% to 20% of that demand,” said Fabian Gerlinghaus, co-founder and CEO of Cellares, a US-based startup that is seeking to revolutionize cell therapy manufacturing.
Cellares co-founders Alex Pesch (left), Fabian Gerlinghaus (center) and Omar Kurdi. All three have earlier worked at genome engineering firm Synthego
Photo Credit: Nancy Rothstein
To put things into perspective, Gerlinghaus explained that in 2020, all cell therapy companies across the globe with a licensed product on the market were able to produce only around 3,000 patient doses, whereas the addressable patient population for CAR-T cell therapies last year was around 450,000 doses.
This huge discrepancy between “what we can make” and “what we need to make” will only exacerbate if one looks at what is in the pipeline, Gerlinghaus said. The number of newly registered cell therapy trials is taking off exponentially with approximately 700 cell therapy trials currently active worldwide.
By 2025, the US Food and Drug Administration expects to approve between 10 to 20 new cell and gene therapies every single year. Consultancy firm McKinsey projects that within the next five to 10 years, the global addressable patient population for CAR-T cell therapies will exceed two million patients per year.
“That's a huge number,” said Gerlinghaus. “If cell therapies can't be made at scale,” patients who need these life-saving therapeutics won’t get access “simply because of the manufacturing bottleneck,” he warns.
How can the production of cell therapies be ramped up to the necessary level? Gerlinghaus believes the best solution lies in automating the entire manufacturing process. “Cell therapy manufacturers are dealing with the same problems across the globe. That's true whether you're in the US, in the EU or in China … The future that we're seeing is definitely a future in which cell therapy manufacturing is fully automated and much more repeatable and robust,” he said.
While there is no fully automated manufacturing platform on the market yet, this situation could soon change.
Gerlinghaus’ own company Cellares, founded in 2019, has developed a fully automated, next-generation cell therapy manufacturing platform called the Cell Shuttle. The platform is a “factory in a box” for industrial scale cell therapy manufacturing that, according to Cellares, offers “true walk-away end-to-end automation.” The platform is a “few short years” away from market launch.
Another company active in this space is Ori Biotech. This London- and New Jersey-based outfit has developed a flexible manufacturing platform that closes, automates and standardizes cell and gene therapy manufacturing. Ori aims to launch its first commercial product in early 2022 and to scale toward a high throughput, fully automated commercial manufacturing system within three years post-launch.
The need for producing cell therapies at mass scale is a relatively recent problem. It arose in 2017 when the first CAR-T cell therapies – Novartis AG’s Kymriah (tisagenlecleucel) and Kite Pharma’s Yescarta (axicabtagene ciloleucel) – were approved by the FDA.
When these approvals came, the industry was using a plethora of benchtop instruments that were never designed for industrial scale cell therapy manufacturing, explained Gerlinghaus.
According to David Smith, vice-president of technical operations at Ori Biotech (North America), to keep up with increasing demand, companies improvised their manufacturing processes by using equipment repurposed from other utilities (e.g., cord blood, stem cells) and retrofitted it for cell and gene therapy manufacturing,
But those were early days. “The majority of the industry has now shifted from manual operations to semi-automated systems,” explained Smith.
There are now several players offering semi-automated solutions targeting different unit operations within the manufacturing process. “Some prioritize automating a single unit operation at a time throughout the development process, while others may automate the full process earlier in development,” said Delara Motlagh of Colorado-based Terumo Blood and Cell Technologies.
There are several tools and solutions available depending on process needs. “For example, there are several automated cell wash/concentration or cell expansion platforms commercially available today; however, the fill and finish step has been primarily manual with recent automated solutions coming to market,” said Motlagh, who is vice-president cell therapy technologies at Terumo.
“The only thing that defines your cell therapy is the manufacturing process. So, we need to give our customers the ability to define their processes.”
Despite recent progress, there are concerns that semi-automated tools do not offer a comprehensive solution. Manual manipulations still exist and this can reduce the effectiveness of scale, robustness, variation and error rates that full automation can bring, said Ori Biotech’s Smith. “The continued need for manual interventions, along with the significant use of consumables, means the reduction in cost of goods for semi-automated [solutions] is modest at only about 10-15%.”
Another problem with some existing semi-automated tools is that they “lock” cell therapy manufacturers into very narrow and rigidly defined workflows. Often that does not work well as “you need to keep in mind that in cell therapy, the process is the product,” said Gerlinghaus.
Companies have little control over the starting material “because the starting material are the cells that you harvest from the patient,” the Cellares executive said. “The only thing that defines your cell therapy is the manufacturing process. So, we need to give our customers the ability to define their processes.”
There is a clear demand for next-generation technology to intensify manufacturing and increase throughput per square feet and both Cellares and Ori Biotech claim that their automated platforms, when launched, will shift the cell therapy manufacturing standard.
Gerlinghaus believes that fully automated manufacturing platforms that close the entire manufacturing process end-to-end can really “change the paradigm here.”
Such platforms can automate the entire process from loading the patient cells, through enrichment, isolation, activation, gene transfer, expansion and the fill-finish process. “What you are going to be unloading at the very end is a cell therapy product that's ready for release testing and infusion into the patient. That's eliminating, most of the human labour,” he said.
Cellares’ Cell Shuttle can produce 10+ patient doses in parallel, which increases manufacturing scalability by an order of magnitude, “which is really what you need to help pioneering cell therapy companies scale out from around a thousand patients to tens of thousands of patients per year per drug,” Gerlinghaus said. This can reduce the per-patient manufacturing cost by up to 70% for most processes.
Another advantage of the Cell Shuttle is that it can be used through all stages of the drug development – from preclinical to commercial stage – which can accelerate market entry of new cell therapies by one to two years, Gerlinghaus explained.
For Ori Biotech, Smith said its first-generation Ori system should allow for savings of ~50% over fully manual operations and ~40% over semi-automated processes. “Once the next generation, scalable Ori system is available, the COGS [cost of goods sold] reductions should be in the order of 60-80% over current processes,” he said.
The cost reductions promised by fully automated platforms come from, among other things, reductions in manual processes, process failures and cleanroom needs.
Gerlinghaus recalls when his company was researching the average failure rates for cell therapy manufacturing, getting precise information from industry was difficult. “It’s like pulling teeth. Nobody likes to talk about it. So, it's very difficult to get hard numbers. My estimate is that it is around 10%,” Gerlinghaus said. “By automating and closing the [manufacturing] process we can achieve a three-fold reduction in process failure rates.”
While automation reduces the risk for operator error, closing the process reduces the risk of contaminating the product. “By eliminating these two primary sources of process failure,” it is possible to reduce the risk of process failure by a factor of three, Gerlinghaus added.
An automated and closed end-to-end manufacturing platform can also significantly reduce cleanroom needs (i.e. the amount of cleanroom space in per square foot that is required per patient) compared to manual methods.
Cellares’ Cell Shuttle maintains its own cleanroom environment. This means it can be deployed in lower class cleanrooms, such as ISO 8 instead of ISO 7 cleanrooms. The former are four to five times cheaper to build and operate per square foot than the latter.
It seems Ori Biotech also has similar plans for its manufacturing platforms. Last November, it collaborated with G-CON Manufacturing, a leader in prefabricated flexible cleanroom solutions, to offer a predesigned platform for flexible manufacturing of cell therapies. Earlier, it also collaborated with Germfree, which provides process-ready, mobile and modular cleanrooms for cell and gene therapies.
There are clearly several arguments in favor of fully- and semi-automated platforms over manual processes, but there are pros and cons to each approach.
When deciding on a manufacturing process, "you have to really think up front about the cost and flexibility,” said Mike Lehmicke, director of science and industry affairs at the Alliance for Regenerative Medicine. “Everyone who is developing a process should ask themselves, ‘What are we doing? How much flexibility do we need? And how much cost is tied up in equipment and clean-room space?’”
Lehmicke also noted that the industry’s increasing focus on allogeneic, or off-the-shelf, therapies should be factored into the equation about automation. With allogeneic therapies, cells can be produced for multiple patients from one donor, which reduces costs even when using manual processes, he noted.
“This is pretty much why all developers have allogeneic pipelines,” said Ori Biotech’s Smith.
Both Cellares and Ori Biotech are currently focused on refining their respective platforms to ensure they meet the varied needs of cell therapy manufacturers.
The Cellares’ platform, for example, supports 85% of cell therapy modalities – both autologous (that uses cells derived from a patient's own body) and allogeneic (that rely on a single source of cells to treat many patients). The platform supports CAR-T, HSC, TCR, NK, TIL, Treg, γδ T cells.
This has been made possible through a “very modular system with a powerful software suite on top” that allows companies to define their own cell therapy processes, said Gerlinghaus. Such flexibility is necessary for a fully automated solution, he added.
Cellares is offering “selected partners” early access to its fully automated manufacturing platform in return for feedback on cell therapy manufacturing workflows and processes. “That puts us in a position where we can ensure that our technology will actually meet their expectations and we'll be able to run and support their particular cell therapies,” Gerlinghaus said.
In January PACT Pharma, a clinical-stage company developing personalized NeoTCR-T cell therapies, secured early access to the platform. In return, it will provide Cellares with insight into autologous NeoTCR manufacturing workflows and participate in user studies.
As for Ori Biotech, it collaborated with Achilles Therapeutics last April to test its cell therapy manufacturing platform. Under the agreement, Achilles will use the Ori platform in its proprietary clonal neoantigen T-cell therapy manufacturing process.
“Standardization [of manufacturing processes] will be vital” if the significant savings that fully automated platforms can deliver are to be realized, said Smith. However, industry to date has been “allergic” to addressing this issue.
This reluctance to standardize processes is due in part to the “biological variation confounded by a lack of disease state material in development and therefore a shortage of understanding [of] the impact of process parameters on critical quality attributes,” Smith explained.
The Ori Biotech executive also believes that, while it may seem contradictory, the standardization of manufacturing processes must be met with a certain flexibility. Smith makes his point by drawing a correlation with an Amazon warehouse, where the orders or inputs are all different, “but automation handles the variation into a standardized platform to produce quality output.”
In cell therapy manufacturing, he explained, every developer does things slightly differently. “Be it cell concentration, bead concentration, culture volume, culture media components, timing of incubation steps… the list goes on,” Smith said. This makes it hard to introduce full automation. If companies opt for flexible automation, “often we turn to well-trained humans as that is cheaper,” Smith explained. So, to realize the full
benefit of automation, “we need to have standardized processes,” but as the biological input is different, “we get into a Catch-22 [situation],” he added.
“Gone are the days of developing disconnected hardware systems that sit on a bench without integrating into the entire process and intensifying manufacturing. Only with this realization, can the industry reduce its costs, increase throughput, increase quality and make these life changing therapies accessible to all,” Smith added.
Industry has to decide between: 1) whether to have a fixed process with variable input and therefore a variable output that offers true personalization, but is hard to regulate; or 2) whether to have a variable process, accommodating variable input for a fixed output that is easier to regulate.
Or “is there an in-between, where you have variable input, variable (but within a design space) process, producing a variable but controlled output? … As an industry we need to understand more about our processes and our inputs to achieve this,” Smith said.
In the area of cell therapy manufacturing, this cannot be achieved through single points of contact, but through integration of the entire value chain to include quality management system, manufacturing execution system, laboratory information management system and enterprise resource planning.
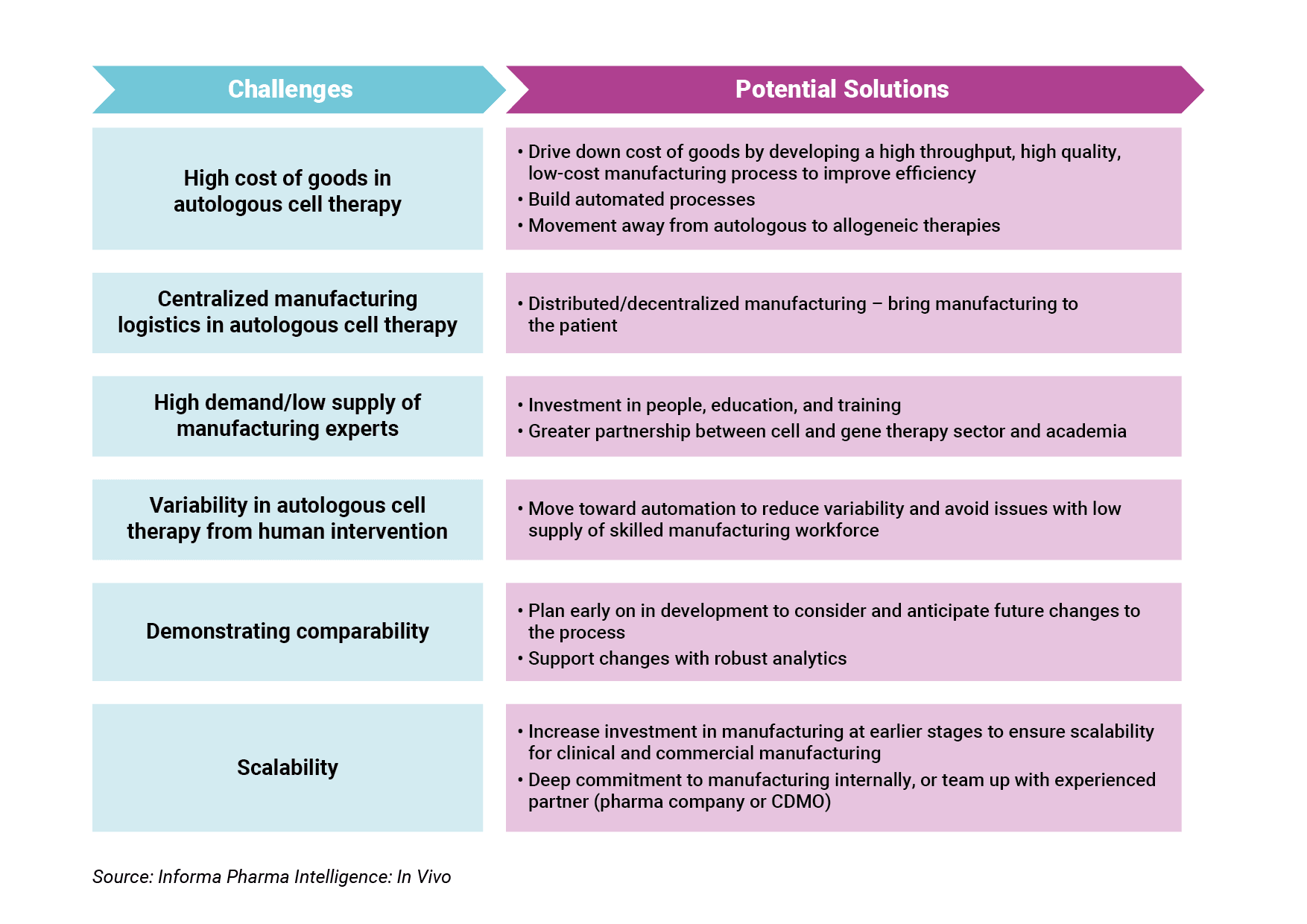
Experts share what they believe are the solutions to key manufacturing challenges, such as lowering cost of goods and centralized manufacturing, in the cell and gene therapy sector.
Regenerative medicines have made significant advancements in patient care, especially for rare diseases and small patient populations who no longer have to fear being told there are no other options. Unlike small molecules and even some biologics, cell and gene therapies have a more challenging road to commercialization and success for many reasons, including the nature of the modality – the promise that some therapies are one-time cures – and the price of such therapies – how do you simultaneously enable patients to access these expensive treatments, but also reward developers for innovation and investment in an arduous research process. These are all critical considerations as predictions have put 40-60 product launches in the US and over 500k patients treated by 2030, according to Peter Marks, the director of FDA’s Center for Biologics Evaluation and Research, and global sales forecasted at $13.23bn by 2023, based on estimates from market research agency ResearchAndMarkets.
Arguably, one of the biggest hurdles in getting cell and gene therapies over the finish line to becoming a sustainable modality on the market is manufacturing. One of the key reasons manufacturing has remained an obstacle is because of the rapid pace of development of cell and gene therapies over the last 10-15 years. “Cell and gene therapy in general is going through this transition from, ‘Is it possible? Is it feasible to?,’ to now, ‘How can it how do we do it?’ That is happening across all of the modalities from the AAV field to even CRISPR/Cas editing, both ex vivo and in vivo, to the cell therapies that we may make, both engineered and un-engineered. I think you're seeing across the board that the realization that it's now about how to do it, not can it be done,” Emile Nuwaysir, president and CEO of BlueRock Therapeutics, told In Vivo. Bayer AG acquired BlueRock in August 2019 for $600m [See Deal], becoming one of Bayer’s bigger investments in the cell and gene therapy field alongside its October 2020 acquisition of Asklepios BioPharmaceutical, Inc. [See Deal] and December 2020 partnership with Atara Biotherapeutics, Inc. [See Deal]. Increased dealmaking and investment in this area resulted in Bayer launching a cell and gene therapy platform in December 2020 operating within the big pharma's pharmaceutical division. (Also see "Bayer Bids To Be A Winner In Cell & Gene Therapy" - Scrip, 8 Dec, 2020.)
In Vivo spoke with Nuwaysir and several other cell and gene therapy manufacturing experts about what they believe are the biggest hurdles for manufacturing in the sector and solutions to those challenges.
Manufacturing has been such a pain point mainly because there was a lack of investment early on in the field, due to wariness about the viability and safety of cell and gene therapies following the death of Jesse Gelsinger, a patient with partial OTC deficiency who received a gene therapy in a clinical trial, in 1999, and cases of leukemia resulting from gene therapy studies in the early 2000s. Even though R&D progressed, manufacturing infrastructure in the sector did not. “Manufacturing technology has lagged so far behind therapeutic development because in the early days of cell therapy, they had a couple clinical trials where patients unfortunately died. And in the early days, the investment community and others got a little bit scared of the potential implications,” Jason C. Foster, the CEO and executive director of Ori Biotech, told In Vivo. Ori was founded in 2015 to provide a bespoke manufacturing platform for cell and gene therapy developers.
In recent years, investment in cell and gene therapy has exploded, with financing for companies in this sector totaling $19.9bn in 2020 according to the Alliance for Regenerative Medicine.
Because of the nature and complexity of these products, cost of goods in cell and gene therapy is extremely high. “The best estimates in the industry is that for the first-generation CAR-T products, cost of goods costs between $150,000 to $200,000 per patient,” said Foster. To reduce this cost, Foster believes the industry needs high throughput, high quality, low cost manufacturing processes, which can be achieved through improvements in automation, robotics and technology.
Cost of goods is central to cell and gene manufacturing, according to Katy Spink, COO and managing partner at Dark Horse Consulting, which specializes in cell and gene therapy products. “It is a near universal issue in my view across the whole field, because the cost of goods of making these things is so high that there's only a business case for the product if it can sustain a pretty high price point,” Spink told In Vivo.
Spink also believes there needs to be automation of manufacturing, and automation in lot release testing for autologous cell therapy manufacturing. “One of the challenges for these patient-specific autologous products is that you have to do individual testing and release of the product for every patient. You don't get to divide that testing cost across the thousands, or tens of thousands of patients per lot the way that you do for traditional small molecule or antibody therapeutics for example.”
Lowering manufacturing costs has a downstream effect on pricing of and access to cell and gene therapies. Enabling and expanding patient access to these medicines will be helped by reducing cost of goods in manufacturing, leading to less expensive methods to make these therapies. The goal is to still allow sponsors to recoup R&D expenses but make medicines affordable for patients. Bringing down cost of goods is also critical if the sector wants to start addressing larger, primary care indications with autologous cell therapy where the value proposition is less extreme. “If we can't figure out how to get cost of goods down, we're just not going to be able to price these therapies at levels that are going to be both affordable and value-based,” said Spink.
Driving down cost of goods could also move cell and gene therapy earlier up in the treatment paradigm, but pricing will still need to validate that investment for a developer, according to Spink. “I'm not advocating for cost-based pricing. I think we're always going to be in a value-based pricing model. But whatever we are pricing the therapy based on value has to have an attractive business proposition for the sponsor.” Spink believes there are certain indications where the value proposition exists to move cell and gene therapy into first-line, but this depends largely on the strength of the safety and efficacy data package.
In the area of gene-modified cell therapies, the shift from autologous to allogeneic has great potential to drive down costs. “Moving to allogeneic allows you to have those economies of scale. You can only eke out so much economy of scale while you’re still in an autologous platform,” said Spink.
Allogeneic therapies have advanced into human testing across a range of oncology indications, and manufacturing experts believe the industry will have a better understanding of the viability of this class soon. “We are reasonably close on [allogeneic]. Actually there are a lot of different approaches being taken – engineering of T cells to make them universal, using gamma delta T cells or NK cells or other approaches – where the underlying immune specificity of the cell is more amenable to an allogeneic approach. I think we've got so many shots on goal right now that are all reasonable from an underlying biology perspective that I'm optimistic that we will get there relatively soon,” Spink stated.
Nuwaysir agrees that availability of allogeneic therapies will make a big impact, and that we should expect to see proof of concept in the near future. “I think [allogeneic therapies] will first be used in places where you don't need stable engraftment, where a transient effect is okay, and the rejection effectively of that therapeutic is okay. BlueRock represents the first in an entirely new category of allogeneic cell therapy where you will see stable engraftment, meaning we've changed the paradigm from a transplant to a biologic. It's one of the biggest sea changes that's happening right now. There's others doing the same sort of thing. I think we'll have the proof point for those in the next few years.”
Centralized manufacturing, in which cells undergo unit operations including genetic engineering at an external location from where the patient is located, is the model for the first generation of autologous cell therapies. There have been reasons for this model, namely to be able to control the process, conducting the process under a quality management system, and having operations and oversight by qualified/skilled personnel.
Centralized manufacturing also increases vein to vein time, though, which is a key consideration for patients who are very sick. “The patients that today have access to some of these therapies are often late-stage, refractory patients. They've failed all the other treatments before, and they've got maybe weeks, not months, to live. And so every day is precious,” said Foster.
Quick View: Cell And Gene Therapy Manufacturing Challenges And Potential Solutions
Foster believes that decentralized, or distributed, manufacturing is key in solving this the issue. The distributed model can bring manufacturing to the patient and remove variability in the process, but there is a critical need to ensure quality and safety. “You could essentially replicate a centralized model, but in a regional hub and spoke model where it's kind of controlled centrally, but you're just actually delivering the manufacturing process in a remote fashion,” said Foster.
Examples include manufacturing pods that sit outside of certified treatment centers that run on the same hardware and software, instruments, and standardized air handling systems, and are monitored in real time and replicate elements of quality control. They would be pre-built turn-key solutions, according to Foster. “You can then assure the regulator and the people who are interested in these issues that you're delivering the same high quality product, with the same safety profile, no matter where the manufacturing is taking place.” To this end, Ori Biotech has partnerships with G-CON and Germfree Laboratories, which are leading players in the modular cleanroom market.
There are still challenges to a decentralized manufacturing solution, says Spink, due to standardization, ensuring the manufacturing is validated from a regulatory standpoint, and finding physical space for the manufacturing. “It is very difficult to have a truly robust and standardized manufacturing process in a distributed model. And it's not just on the manufacturing, it's also the characterization and release,” says Spink. Instead, Spink believes automation in centralized manufacturing should be fine-tuned first before shifting toward decentralized approaches.
Highly trained and skilled manufacturing professionals are high in demand but low on supply. This is a big concern in the cell and gene therapy sector, especially for early-stage companies that might be inexperienced in the manufacturing component, leading to issues down the road. Yatindra Tirunagari, head of production DSP at Rentschler ATMP Ltd., told In Vivo, “Currently one is witnessing a surge in small and mid-sized drug development companies entering the CGT space and trying to generate phase I, II and III material. While these new entrants may understand the drug, they may not fully understand manufacturing and are inexperienced in CMC requirements, as well as in handling complexities within the projects. This can lead to errors and even ‘small’ errors in this early phase can have ‘huge’ and expensive consequences at a later stage.” In February 2021, Rentschler Biopharma announced it was establishing their ATMP development and manufacturing capabilities at the Cell and Gene Therapy Catapult’s site in Stevenage, UK.
Finding skilled workers is also a concern for niche and early-stage modalities within cell and gene therapy. “There are no pre-trained people in my field. I'm even earlier in development than even the AAV field. So there is none. We effectively have to train that staff for that narrow discipline,” said Nuwaysir.
The solution to this issue is to make a commitment to investing in people, education, and training to find the right operators to staff. “The industry cannot solve [this issue] without investing into education of people. People will not just fall from the sky and not everybody will just be enthusiastic about cell and gene therapy as we are. Investing into people and capabilities, I think personally, is absolutely crucial,” Wolfram Carius, executive vice president and head of Bayer’s Cell & Gene Therapy Unit, told In Vivo.
Tirunagari believes there should be greater partnership between the cell and gene therapy sector and academic institutions. “Talent shortage can only be resolved when academia and industry collaborate and cooperate to this end. Solutions for bridging the talent gap include hands-on training programs for bioprocessing and cell and gene therapy, industry-academia collaborations, and internships or fellowship opportunities to nurture talent.”
Even with qualified and skilled personnel, human intervention can lengthen the time it takes for the genetic programming and the cell expansion steps in autologous cell engineering, and subsequently increases the risk for errors in those steps. According to Foster, this is a big piece of the logistics hurdle that needs to be fixed. Variability is introduced into the process by humans, leading to therapies coming out of specification. “We see a lot of variability because we, as human beings, no matter how skilled we are, introduce variability into manufacturing processes because we just don't do it as reliably as a robot can.”
Foster says the industry needs to remove or reduce human intervention by moving toward automation, not only to improve variability, but also to address the supply issue of experienced manufacturing professionals. “There just aren’t enough of these highly skilled operators that you need. This move to automation has to be done to fill that gap.”
According to Spink, changing manufacturing is a common practice among cell and gene developers. But demonstrating comparability after there are changes to a manufacturing process is a key issue and is closely integrated with other important metrics. “I would tie analytical characterization and measurement of potency as being important, related, and overlapping issues with comparability.”
Problems with comparability have been the cause for many of the setbacks in the cell and gene therapy sector, according to Anthony Davies, founder and CEO at Dark Horse Consulting. “If you look at some of the recent failures and delays, a disproportionate number tracks to asset development, and a disproportionate number of those tracks to potency,” Davies told In Vivo.
To avoid pitfalls with comparability, manufacturing experts who spoke with In Vivo advise planning early on in development to be flexible enough to consider and anticipate future changes to the process. “Begin with the end in mind. Think from day one about what you want your commercial process to look like, plan ahead for future changes you are going to have to make to get there, and make sure that they are ones that will be manageable at that stage of development,” said Spink.
Any type of changes to the manufacturing process should be supported by strong and robust analytics to ensure process changes have not altered the final product, an important consideration not only for the developer, but also for regulators. “When you are dealing with products with complex mechanism mechanisms of action, you have to deal with complex analytical challenges and complex analytical methods,” said Davies.
Spink believes that there will be big developments in analytical technologies. “As our analytical technologies advance, it's going to greatly facilitate that issue. There are things like single cell RNA seq[uencing], for example, that weren't available a decade or so ago that are today, that are still not suitable as validated release assays but that can be used on a product characterization basis to help us think deeply about product comparability.”
Most manufacturing for cell and gene therapies has originated in academic labs, which each have their own processes they have developed at a small scale, or what Foster refers to as their “secret recipe.” Lack of investment in manufacturing has led to processes that end up being difficult to scale for eventual commercialization. “[Academic labs] don't necessarily have the ability or take the time to try to prepare the process for scale. They want to make sure that it's safe for patients, and that it can make it into the clinical trial process. But they're not thinking about hundreds of patients or certainly not thousands of patients at that stage,” said Foster.
Many issues that exist in the cell and gene therapy field currently relate to scalability, according to Tirunagari. “Firstly, separate platform technologies are currently being applied for each individual vector. This obviously translates to added effort and costs. Secondly, one is faced with the challenge of low productivity owing to the very complex nature of the end product. Existing technologies are not yet future proof and transient transfection must be established as a scalable model. Thirdly, limited regulatory guidance and product complexity deepen analytical challenges.”
Spink agrees that scalability has been the core reason for disappointments in the sector. “Many cell and gene therapy products failed – either in late-stage clinically, or just failed to actually be viable commercial products even once they were approved – because they were very academic, unscalable processes, and possibly not reproducible processes as well, that were then sustained throughout development rather than improved because people were so scared to change the process because of concerns about comparability.”
Manufacturing to commercial scale is especially difficult for small biotechs that do not have deep expertise,
commitment, and financial resources. “The decision on how to go to the next step, how to manufacture for commercial scale – that’s not something that you can do easily as a standalone biotech. It's not only not easy to finance, but it's also very difficult to staff from an expertise point of view, and to have the vision to do it,” said Nuwaysir.
Addressing the issue of scalability will require marked changes in the industry, stated Tirunagari. “Currently, manufacturing processes are transferred from academia and these are not yet robust for industrial scale up. We need to transform these processes and not just improve them.”
One of the keys to achieving this transformation is through increasing investment in manufacturing at earlier stages to ensure scalability for clinical and commercial manufacturing. This also entails planning for and anticipating changes that may alter the final product. “The process – on the CMC development, on developmentability, on scalability, on manufacturability – determines not only efficiency, but has an impact on safety, and has a clear impact on the quality or reproducibility of a product,” said Carius, who stated that this is a largely different mindset than development of traditional pharmaceuticals. “Thinking through the value chain from the very beginning – thinking about raw materials, of the raw materials of the raw materials, and the impact on the processes as well as the production strategy, the entire part of primary, secondary equipment or even material where you store package freeze – has an extraordinary importance compared to what you classically do in pharma.”
Success in scalability requires a cell and gene therapy developer to have a strong commitment to internal manufacturing. If that is not an option, as Nuwaysir explains, partner with an experienced company that has the resources. “To have the vision to do it, that’s something that’s better suited for a partnership with a little company like BlueRock and a big company like Bayer, who's shown a long history of expertise and commitment in the space…its Bayer providing that other expertise and building that facility with us as the user, helping to direct the specifications. It’s not just about the narrow role of the operator, it's about the entire team,” said Nuwaysir.
In addition to big pharma, there are many advantages for companies to partner with an experienced CDMO, according to Tirunagari. “Working with a CDMO can offer a competitive edge to small and mid-sized companies, for example those that have a limited pipeline catering to rare and ultra-rare diseases. Capacity constraints can be resolved through innovative manufacturing set-up and operations.”
Many companies are working toward addressing key manufacturing challenges in cell and gene therapy with these solutions. Further, long awaited investments in manufacturing have been happening and picking up pace. One clear sign is the uptick in dealmaking activity by cell and gene manufacturers over the last two years. (Also see "Gene Therapy Manufacturers Are Highly Sought Acquisition Targets" - In Vivo, 9 Dec, 2019.) Expanding manufacturing capacity remains an obstacle and is a big driver of these acquisitions. For that reason, consolidation is expected to continue. “I think there will be expansion, there will be carve-outs, there will be buy-outs. From where I sit, it’s increasing, not decreasing,” said Davies.
Nuwaysir agrees there is a capacity crunch that will fuel dealmaking in manufacturing. “For the foreseeable future, as far as we could imagine, demand will outstrip supply. The only question is, is the price the right price for the acquirer? So it makes some acquisitions more or less attractive.”
Some of the largest deals in the cell and gene therapy sector so far in the first quarter of 2021 were for cell and gene therapy manufacturers – Charles River Laboratories International, Inc.'s $875m purchase of Cognate BioServices Inc.; Novasep Holding SAS's €725m sale of Henogen to Thermo Fisher Scientific; and WuXi AppTec Inc.'s completion of a $135m takeover of OXGENE – all positive signs for this industry.
Merck & Co. executive outlines how the company could sustain a “compliant supply performance” amid the pandemic, while senior officials from Sun Pharma, Cipla, Zydus Cadila and Biocon shared insights on coping with supply chain turbulence and moving away from over-dependence on China for starting materials.
Senior executives from Merck & Co., Inc. and several leading Indian pharma firms have shared insights around how they built supply chain resilience against the backdrop of the general turmoil during the early days of COVID-19. The experiences were also dotted with interesting real world vignettes, including the hijack of a pharma cargo truck in India.
Addressing the recently concluded BioAsia 2021 virtual event, Sanat Chattopadhyay, executive vice-president and president, Merck Manufacturing Division, noted the pandemic had unleashed a “tsunami” of changes, causing an inflection point in the life sciences segment . Industry, he said, is now innovating how it “designs, executes and risk manages” supply chains.
Chattopadhyay said that throughout the pandemic Merck had managed to maintain a “compliant supply performance” without adding inventory or increasing discards, attributing that robustness to certain capabilities built up over the last three to five years, including end-to-end supply planning.
“We have been digitizing our shop floors end-to-end from raw materials, drug substance manufacturing, formulation, packaging, testing and release. This capability has been critical to navigate challenges,” the executive said in his keynote address at the online event, usually held in Hyderabad each year.
Some other important measures at Merck included putting in place a “control tower”, facilitating real time planning. Sales and operations planning was no more a once-monthly exercise but rather such activity happened weekly and enabled real-time action. For example, during the pandemic Merck could divert vaccines from Japan to Germany within a week - in the past it would have taken at least three months to accomplish this, Chattopadhyay observed.
The US company is also transforming its distribution and logistics operations to be more digital, using cloud-based processes. It is tracking high-value shipments in real time with IoT (internet of things) connected devices and also innovating its cold chain container systems on an ongoing basis.
“From a pandemic standpoint, as airports closed and ports became congested, we were able to track and divert our shipments in real time with the help of our freight partners,” Chattopadhyay explained, adding that the company has also developed an enterprise-level event management process.
Outlining some of the key lessons for pharma from the pandemic, the executive emphasized the need to keep accelerating the "digital journey" for supply chains – making sure the process is much more end-to-end and as close as possible to real time – in addition to agility.
Another critical aspect is to accelerate risk management transformation, ideally expanding the scope of this to include tier 5 suppliers, like the aerospace and chip industries have learnt to do. Pharma’s outreach beyond tier 2 during the pandemic was often manual and time consuming, he observed. (Primary direct suppliers are tier 1, with subsequent tiers defining those further down the indirect chain and which may supply those further up.)
“The smallest component from a tier 4 or 5 supplier could be the Achilles heel in an otherwise healthy global supply chain of a global pharma company,” Chattopadhyay said. Experts have previously highlighted the exponential complexity of global supply chains, with most large organizations having little idea of who their tier 2 or top 10 critical tier 2 suppliers are.
The BioAsia conference also saw senior executives from top Indian firms discuss key aspects around supply chain disruption and ensuring stability amid COVID-19 related turbulence.
The initial months of the pandemic outbreak last year were clearly chaotic. Gaurav Suchak, head of supply chain at Zydus Cadila, recounted how there was no clarity in terms of what lay ahead at the time, with some manufacturing sites closed, firms grappling with how to keep plants running and with moving labor from one place to another. (Also see "COVID-19 Lock-Down: India Pharma Manufacturing Limps Along Amid Challenges" - Scrip, 8 Apr, 2020.)
“There was a stand-still in terms of global trading logistics as well. What was missed the most at that time was end-to-end supply chain visibility,” Suchak said on a panel discussion during the conference.
He emphasized the key role and prompt response of the Indian government machinery in addressing various “pain points”. This ensured that within a couple of weeks of the first lock-down in India the company was “good in terms of how we were able to sail through” and get things up and running. Teams rallied around the larger cause of ensuring supplies of life-saving drugs and within no time switched to a digital way of working.
“All in all industry was able to respond to the disruptions very well,” Suchak said.
Other experts within the Indian industry brought in additional interesting dimensions, outlining the extent to which pharma companies went to sustain steady supplies. Sreenivas Rao, global head, supply chain at Sun Pharmaceutical Industries Ltd., India’s top-ranked drug maker, said the firm tried to put end-to-end supply chain visibility on a dashboard to help identify the weak links.
While some “panic buying” of raw materials was required, the firm also pressed upon the resources required, even as it meant an increase in inventory and the “worsening” of working capital, though those aspects were considered secondary at the time. Other initiatives included starting sales and execution cycles on a weekly basis.
Rao also recalled how, towards the end of June last year when flights were grounded, the firm went ahead and chartered a flight, deploying a passenger plane for cargo supplies. The flight apparently flew in almost empty and flew out with 11 Unit Load Devices of material and entailed "a ton” of money.
“But at the end of the day that was very important for us to save lives in various parts of the world,” Rao explained.
The executive underscored that the most critical components remained the safety of workers and “creating pride” in employees in the factory and supply chain, to show that they weren’t working only to make a living for themselves but were "Corona Warriors".
Rao also highlighted the value of digitization, throwing in a real-world example of the hijack of one truck carrying Sun’s goods in the Indian state of Bihar around a month ago. He noted that while a book worth INR100 ($1.40) ordered on Amazon can be tracked because of digitization – the complete history of the shipment is available – such real-time tracking is lacking in the case of trucks carrying pharma goods.
“I got to know of the hijack of the truck carrying goods worth a crore of rupees [about $137,600] after 2.5 days. That’s very sad in my opinion. The whole truck is moving with crores of rupees worth of goods and we don’t have that digitization to that effect, but a small courier packet which is carrying a book worth INR100 has a whole lot of digitization,” he said during the panel discussion.
Had things been optimally digitized, there would have been information available that the truck had been “standing for 2.5-3 hours more than it should be” and also a mobile alert indicating that it wasn’t going via its regular route. This could have then helped alert officials in the region to make sure the hijacking was tackled promptly. Even some under-developed countries in Africa that have higher incidents of theft have seen higher digitization and already have such systems in place, he noted.
Rao also believes that pharma could more broadly do with a significant infrastructure upgrade, whether it be warehouses or clearing and forwarding agents, and noted that things are moving rapidly in the external environment. For example, large groups have bought distributors. (Also see "Asia Deal Watch: Takeda Will Employ Engitix’s ECM Tech In Liver Fibrosis Indications" - Scrip, 25 Aug, 2020.)
“If we don’t digitize we’ll soon become history," he warned. "COVID-19 has expedited digitization, we should embrace it and run it like a relay race.”
Panelists at BioAsia also discussed the broader trend around Indian firms moving to de-risk supply chain linkages with China, with various strategies still being worked out.
“For critical active pharmaceutical ingredients [APIs], companies are keen to consider backward integration so that you are in control of that pie that is going to make the most impact on your business and also make sure that the entire value chain is secure,” Zydus Cadila’s Suchak said. (Also see "Early API Momentum At Indian Firms: Not Just A Quarterly Bump?" - Scrip, 27 Jul, 2020.)
Qualifying multiple vendors or identifying local vendors with good quality and consistency in supplies at competitive prices are other options being pursued.
Prasad Deshpande, global head of supply chain at Biocon, Ltd., indicated that the company has a metric around what percentage of its revenue is “independent” of China. “By the last quarter we were almost 50-60% independent of China. [This] doesn’t mean we can’t source from China, but we are not dependent on China anymore,” he commented. (Also see "How India API Manufacturing Stacks Vs China, Addressing Challenges" - Scrip, 24 Apr, 2020.)
Swapn Malpani, joint president and global head, supply chain, Cipla Limited, indicated that the firm has initiated an "API Reimagination" plan that has multiple levers, including efforts to ensure that internal manufacturing capacities are ramped up. He noted that there are multiple schemes launched by the Indian government supporting API production and that the company was actively looking at some of these. (Also see "India APIs Incentive Scheme: Will It Galvanize Local Firms, Bridle The Dragon?" - Pink Sheet, 8 Jun, 2020.)
“We are also looking at how we can go to some of the CMOs [contract manufacturing organizations] in India and de-risk our channel, particularly intermediates, and there are some good capabilities existing in India,” he added.
China is currently estimated to account for over 60% of total imports of APIs and intermediates into India, though this has not always been the case. The Indian bulk drugs segment was actually ahead of China until the 1990s.
Resilience has raised $800m to develop new technologies to manufacture complex drugs including vaccines, cell therapies and gene therapies.
National Resilience Inc., a new company backed by a rich $800m investment and an impressive leadership pedigree, aims to tackle next-generation biopharma manufacturing challenges, starting in 2021. The company will focus on developing new technologies to manufacture the most complex medicines including cell and gene therapies, viral vectors, vaccines and proteins.
"We are working on technology that is disruptive. It's not just process-development of existing platforms," CEO Rahul Singhvi said in an interview. "We actually look more like a special force, or a problem-solving unit, than a [contract manufacturing organization]."
Singhvi was lured away from Flagship Pioneering to take the CEO position, attracted by the lucrative financing and stellar team being assembled by ARCH Ventures founder Robert Nelsen. Resilience announced a $750m Series A financing on 23 November, bringing its total financing to $800m. Nelson is chairman of the company's board, and ARCH led the investment, whose participants also included 8VC, GV (formerly Google Ventures) and NEA, as well as some foundations, mutual funds and US-based pharmaceutical companies.
Former Juno Therapeutics Inc. executive Patrick Yang is vice chairman and Sandy Mahatme, former Sarepta Therapeutics, Inc. CFO, is president, chief operating officer and CFO. The company's board of directors includes impressive names like former Bill & Melinda Gates Foundation CEO Susan Desmond-Hellmann, former US Food and Drug Commissioner Scott Gottlieb, California Institute of Technology professor and Nobel Laureate Frances Arnold and more.
Singhvi got a phone call from Yang about the opportunity in June and was intrigued by the opportunity as someone who had been watching the increasing gap between developments in innovative therapeutics and developments in manufacturing. Before Flagship, he worked at Takeda Pharmaceutical Co. Ltd. as COO of vaccines and was the CEO at Novavax, Inc..
"COVID-19 was the lightning rod for folks like Bob Nelsen and others to make this a priority," Singhvi said. "I think it became obvious to them…[that] manufacturing is a real big pain point so that served as the catalyst to drive this company."
Resilience has already acquired one contract manufacturing organization and is acquiring a second, both of which are located in either the US or Canada.
"We are in the process of acquiring a number of different technologies and building the laboratories," Singhvi said. "In parallel, we feel it is very important for us to have experience with customers, so we have also acquired companies that are already operating and already interfacing with customers, so we can get the business started."
Resilience expects to be producing orders in early 2021, but new technology solutions will come later toward the end of the year. The parent company employs 25 people currently, but the two acquisitions will bring in another roughly 550 employees.
Other critical areas the company hopes to improve upon is tech transfer and capacity constraints, so that innovations can be developed faster. The wait time to bring new products online can be lengthy – sometimes up to six to 12 months, which can be critical time for a startup that is burning cash, Singhvi said.
"If you are able to give them capacity sooner, then hopefully that would also be valuable to our customers," he added.
The initial focus is to create a network of manufacturing facilities and laboratories in the US and Canada, an issue COVID-19 put into stark clarity with early concern about the potential for drug shortages and then lack of capacity for manufacturing novel antibodies and vaccines.
"Part of our goal is to solve this double bottom line thing, that we have to be sustainable as a business by solving a market need, but have this infrastructure available in the US so that if we have to then pivot to making vaccines or something else…that we can do that," Singhvi said.